コンテンツへスキップ
About Us
Message from CEO
Our Mission
Company Profile
Management Team
History
Clinical Development
Ongoing Clinical Studies
MN-166 (Ibudilast)
About MN-166 (Ibudilast)
ALS
Oncology / Glioblastoma
DCM
CIPN
ARDS / Lung Injury
MN-001 (Tipelukast)
About MN-001(Tipelukast)
NAFLD, Type 2 Diabetes Mellitus, and Hypertriglyceridemia
Investor Relations
Press Release
Event
Media Archive
Annual Report
SEC filing
Stock Quote -TSE
Stock Quote -Nasdaq
Historical Price Lookup
Investment Calculator
Analyst Coverage
Corporate Governance
Information Request
Presentation
Corporate Presentation & Resarch Reports
MN-166 Presentation
Progressive Multiple Sclerosis (Progressive MS)
Amyotrophic Lateral Sclerosis (ALS)
Oncology / Glioblastoma
Substance Dependence and Addiction
MN-166 (ibudilast) News Articles
MN-166 (ibudilast) Publications
MN-001 Presentation
Contact Us
Contact Us
Japanese site
About Us
Message from CEO
Our Mission
Company Profile
Management Team
History
Clinical Development
Ongoing Clinical Trial
MN-166 (Ibudilast)
About MN-166 (Ibudilast)
ALS
Oncology / Glioblastoma
DCM
CIPN
ARDS / Lung Injury
MN-001 ( tipelukast)
About MN-001(Tipelukast)
NAFLD, Type 2 Diabetes Mellitus, and Hypertriglyceridemia
Investor Relations
Press Release
Event
Media Archive
Annual Report
SEC filing
Stock Quote -TSE
Stock Quote -Nasdaq
Historical Price Lookup
Investment Calculator
Analyst Coverage
Corporate Governance
Information Request
Presentation
Corporate Presentation and Equity Research Analyst Reports
MN-166 Presentation
Progressive Multiple Sclerosis (Progressive MS)
Amyotrophic Lateral Sclerosis (ALS)
Oncology / Glioblastoma
Substance Dependence and Addiction
MN-166 (ibudilast) News Articles
MN-166 (ibudilast) Publications
MN-001 Presentation
Contact Us
Home
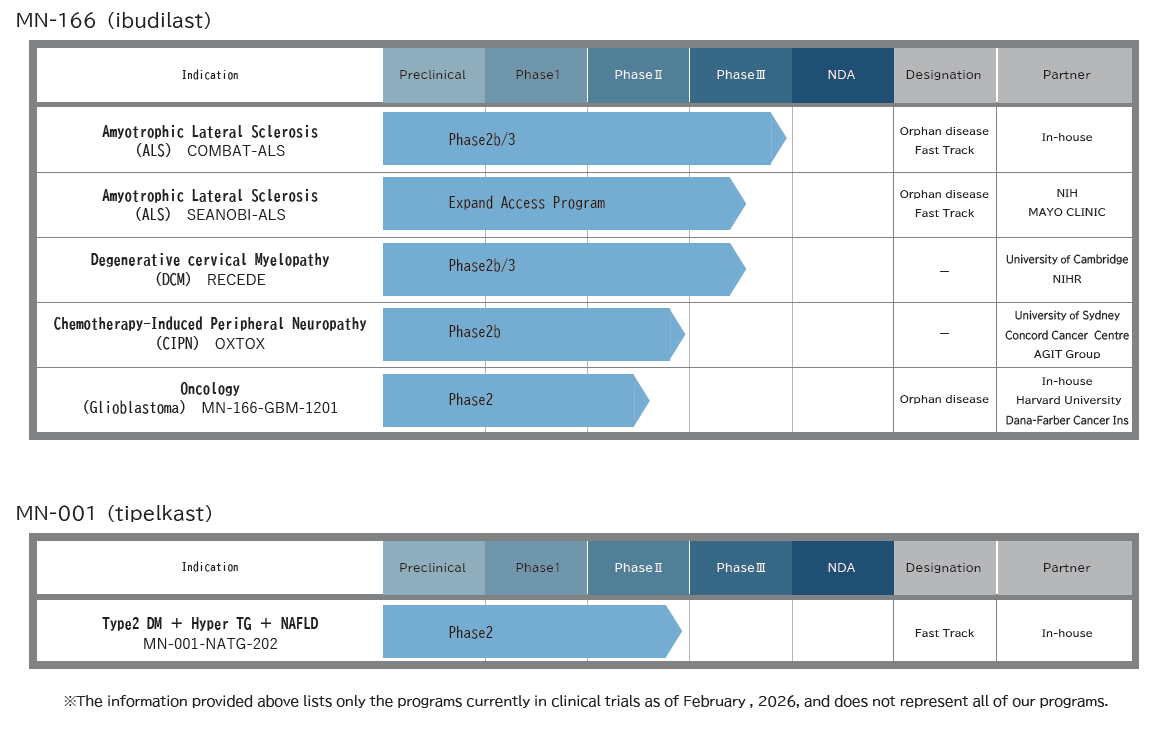
Ongoing Clinical Trial
Ongoing Clinical Trial
2017.10.11
2026.03.19
メニュー
About Us
Message from CEO
Our Mission
Company Profile
Management Team
History
Clinical Development
Ongoing Clinical Trial
MN-166 (Ibudilast)
About MN-166 (Ibudilast)
ALS
Oncology / Glioblastoma
DCM
CIPN
ARDS / Lung Injury
MN-001 ( tipelukast)
About MN-001(Tipelukast)
NAFLD, Type 2 Diabetes Mellitus, and Hypertriglyceridemia
Investor Relations
Press Release
Event
Media Archive
Annual Report
SEC filing
Stock Quote -TSE
Stock Quote -Nasdaq
Historical Price Lookup
Investment Calculator
Analyst Coverage
Corporate Governance
Information Request
Presentation
Corporate Presentation and Equity Research Analyst Reports
MN-166 Presentation
Progressive Multiple Sclerosis (Progressive MS)
Amyotrophic Lateral Sclerosis (ALS)
Oncology / Glioblastoma
Substance Dependence and Addiction
MN-166 (ibudilast) News Articles
MN-166 (ibudilast) Publications
MN-001 Presentation
Contact Us
検索